Kevin S. Barlotta, MD
University of Alabama at Birmingham (UAB)
Chief Complaint: Left groin pain and swelling.
HPI: 29-year-old male smoker presents to the emergency department 4 days after treatment for urethritis with intramuscular Rocephin and oral Azithromycin. Patient endorsed high-risk sexual exposure (unprotected vaginal intercourse) 6 days prior to initial presentation and treatment. HIV and RPR testing were negative. N. gonorrhoeae and Chlamydia DNA testing were positive. Patient denied subsequent sexual exposure or masturbation. He noted initial improvement of his symptoms with subsequent development of left groin pain, penile swelling and discharge. He endorsed subjective fever and chills. Review of systems was negative for abdominal and musculoskeletal complaints. No rash, eye or oropharyngeal symptoms were present.
Physical Exam: 113/74 100 99.8 18 95% RA
- General: Alert, mild discomfort, no acute distress.
- Skin and genitourinary: No petechiae. Swelling noted along the penile shaft with clear drainage from urethral meatus. Palpable left groin lymphadenopathy with noted erythema and tenderness (Figure 1).
Significant diagnostic results:
- Glucose: 102 mg/dL
- WBC 5.9 103/cmm
- ESR: 29 mm/hr
- CPR: 1.94 mg/L
- Lactic acid 1.1
- Urinalysis: Yellow, hazy, Specific gravity 1.031, pH 5.0 1+ protein, Trace leukocyte esterase, negative nitrite, 10 RBC/HPF and 42 WBC/HPF. Urine culture 0 CFU/ML.
Questions:
- What diagnosis should you entertain in the setting of progressive sexually transmitted infection?
- What is the appropriate duration of therapy?
Figure 1: Inguinal exam

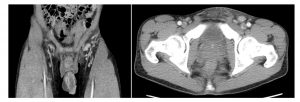
Figure 2: CT abdomen and pelvis
- Focal swelling along the right aspect of the shaft of the penis with associated enhancement of the Buck’s fascia.
- Subcutaneous stranding within the pre-pubic soft tissues and left inguinal region with associated reactive left inguinal adenopathy
Answers:
- Lymphogranuloma venereum (LGV).
- Doxycycline 100 mg oral twice daily for three weeks.
Discussion:
Lymphogranuloma venereum is a disease caused by 3 unique strains of Chlamydia trachomatis (L1, L2 or L3 serovars) and is characterized by a small, often asymptomatic skin lesion (self-limited genital ulcer) followed by regional lymphadenopathy in the groin or pelvis.
The most common clinical manifestation in heterosexuals is unilateral, tender inguinal and/or femoral lymphadenopathy (aka regional lymphadenopathy). Patients with rectal exposure may present with proctocolitis which can mimic inflammatory bowel disease and cause a mucoid and/or hemorrhagic rectal discharge, anal pain, constipation, fever, and tenesmus. There is a risk of developing chronic colorectal fistulas and strictures as well as an invasive systemic infection and a reactive arthropathy. Treatment is Doxycycline 100 mg twice daily for 21 days (or Erythromycin 500 mg QID for 21 days). Test of cure is recommended 3 weeks after completion of treatment, especially in pregnant females. Recognition and appropriate treatment duration are essential to avoiding complications. Education and activity modification are essential to avoid spread and reinfection. Reporting to the state health department is required.